
Overview
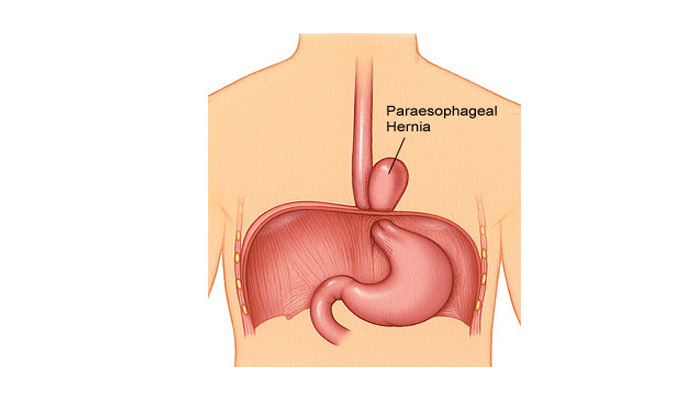
The paraesophageal hernia is less common but is more cause for concern. In many patients, paraesophageal hernias may not cause any symptoms. These asymptomatic paraesophageal hernias can be safely observed and do not require surgery. When a paraesophageal hernia begins to cause symptoms (chest pain, upper abdominal pain, difficulty swallowing), these are usually repaired.
Symptomatic paraesophageal hernias are at higher risk for progressing to incarceration (stomach gets stuck resulting in obstruction) or ischemia (blood supply to the stomach is cut off) resulting in the need for emergency surgery. For expert evaluation and treatment, consult Dr. Ujwal Zambare, a leading GI Surgeon & Gastroenterologist in Wakad, Pune
Common Symptoms of Paraesophageal Hernia
More than half of the population has a hiatal or paraesophageal hernia. However, most people are symptom free. Hiatal hernias and paraesophageal hernias may cause symptoms such as reflux and heartburn; nausea, burping, and vomiting; regurgitation of food; unexplained upper abdominal or chest pain; a sense of fullness after eating; bloating; shortness of breath or coughing; or a sense of food getting stuck in the chest. Severe symptoms occur when the bowel or stomach twists or loses its blood supply. These include heart racing, palpitations, shortness of breath, chest pain, severe vomiting, lack of bowel movements, and severe abdominal pain. These symptoms require immediate medical attention.
Diagnosis
A paraesophageal hernia may be incidentally identified during imaging such as chest x-ray, computed tomography (CT), or magnetic resonance imaging. Patients with symptoms may undergo barium swallow, in which a contrast agent is swallowed and a series of x-rays reveal the anatomy of the esophagus and stomach. An upper endoscopy (esophagogastroduodenoscopy) is a procedure done under sedation in which the doctor visualizes the anatomy of the esophagus and stomach by inserting a thin camera to look at the upper gastrointestinal tract. Manometry may be used to measure the severity of the disease and to establish treatments. This is a study that allows the pressure inside the esophagus to be measured to determine if the muscles are too loose or too tight. A CT scan may be used for surgical planning.
When Should a Paraesophageal Hernia be Repaired?
In general, all paraesophageal hernias causing symptoms should be repaired. Common symptoms from a paraesophageal hernia include:
- Chest pain—there are many causes for chest pain. It is important that patients who have a large paraesophageal hernia with chest pain undergo some kind of a cardiac evaluation to make sure that the chest pain is not from their heart. Typically, eating brings on chest pain from a paraesophageal hernia. Some patients have pain every time they eat, and others only experience discomfort every once in a while.
- Epigastric pain—this is pain in the middle, upper abdomen.
- Dysphagia—difficulty swallowing.
- Shortness of breath—in some very large paraesophageal hernias, the stomach may push on the diaphragm or compress the lungs contributing to a sensation of shortness of breath. There are many other reasons for shortness of breath in addition to a paraesophageal hernia.
- Early or prolonged satiety—Because the stomach is twisted or compressed due to the hernia, it may be difficult for patients to eat a normal sized meal. Patients may feel full for a very long time after eating, which is due to the fact that the stomach can’t empty normally when it is herniated. Some patients may lose weight because of difficulty eating.
- Stomach ulcer—in some patients with paraesophageal hernias, the stomach may twist upon itself resulting in a specific kind of stomach ulcer known as a Cameron’s erosion. These ulcers can occasionally contribute to chronic slow blood loss and anemia.
How are Paraesophageal Hernias Repaired?
Almost all paraesophageal hernias can successfully and safely be repaired laparoscopically (with about 5 very small incisions) and through the abdomen (rather than the chest cavity). The laparoscopic repair of large paraesophageal hernias (most of the stomach resides above the diaphragm in the chest cavity) is a complex procedure and should only be attempted by expert laparoscopic surgeons with extensive experience in laparoscopic foregut surgery. During surgery, the stomach is gradually moved back into the abdominal cavity. The diaphragm at the esophageal hiatus is closed to prevent the stomach from re-herniating. In some cases, a special kind of mesh is needed to close the diaphragm appropriately. Once the diaphragm has been closed, most patients undergo a fundoplication or a ‘wrap’ similar to what is done for a patient with GERD. The fundoplication is performed to help keep the stomach from herniating back into the chest cavity.
Schedule Your Consultation Today!
If you’re experiencing symptoms of a paraesophageal hernia, don’t wait for complications to arise. Dr. Ujwal Zambare, renowned Hernia Specialist and Gastroenterologist in Wakad, Pune, provides expert diagnosis and advanced treatment options.